Cost of the operation
Correction
K01
Correction of nipple retraction under local anesthesia on one side (general anesthesia is paid additionally)
18 000 ₽
K02
Correction of nipple retraction under local anesthesia on both sides (general anesthesia is paid additionally)
30 000 ₽
K03
Reduction of one areola under local anesthesia (general anesthesia is paid additionally)
35 000 ₽
K04
Reduction of two areolas under local anesthesia (general anesthesia is paid additionally)
50 000 ₽
Who needs correction?
The appearance of a woman's breasts can change under the influence of many factors: hormonal fluctuations, expecting a child and lactation, sudden weight loss, previous surgeries, mastitis. In this case, changes can also negatively affect the condition of the nipple-areolar complex. Correction of nipples in a specialized medical setting can be carried out either separately or in combination with a breast lift. Mammoplasty of the nipple and areola is recommended in the following cases:
- with asymmetry;
- in case of acquired deformity;
- for correction of elongated, retracted, widened nipple;
- with complete and partial absence;
- due to the large area of the areola;
- in case of violation of pigmentation of the areolar area.
The photo shows the result before and after surgery. Breast areola correction. Plastic surgeon – D. G. Chepezubov
Photos before and after
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Lobachev Kirill SergeevichLobachev Kirill Sergeevich https://www.bustclinica.ru/doctors/lobachev-kirill-sergeevich/
Chepezubov Denis GennadevichPlastic surgeonhttps://www.bustclinica.ru/doctors/chepezubov-denis-gennadevich/
Chepezubov Denis GennadevichPlastic surgeonhttps://www.bustclinica.ru/doctors/chepezubov-denis-gennadevich/
Chepezubov Denis GennadevichPlastic surgeonhttps://www.bustclinica.ru/doctors/chepezubov-denis-gennadevich/
Chepezubov Denis GennadevichPlastic surgeonhttps://www.bustclinica.ru/doctors/chepezubov-denis-gennadevich/
Chepezubov Denis GennadevichPlastic surgeonhttps://www.bustclinica.ru/doctors/chepezubov-denis-gennadevich/
Chepezubov Denis GennadevichPlastic surgeonhttps://www.bustclinica.ru/doctors/chepezubov-denis-gennadevich/
Chepezubov Denis GennadevichPlastic surgeonhttps://www.bustclinica.ru/doctors/chepezubov-denis-gennadevich/
Chepezubov Denis GennadevichPlastic surgeonhttps://www.bustclinica.ru/doctors/chepezubov-denis-gennadevich/
Chepezubov Denis GennadevichPlastic surgeonhttps://www.bustclinica.ru/doctors/chepezubov-denis-gennadevich/
Chepezubov Denis GennadevichPlastic surgeonhttps://www.bustclinica.ru/doctors/chepezubov-denis-gennadevich/
Chepezubov Denis GennadevichPlastic surgeonhttps://www.bustclinica.ru/doctors/chepezubov-denis-gennadevich/
Chepezubov Denis GennadevichPlastic surgeonhttps://www.bustclinica.ru/doctors/chepezubov-denis-gennadevich/
Chepezubov Denis GennadevichPlastic surgeonhttps://www.bustclinica.ru/doctors/chepezubov-denis-gennadevich/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Saitova Sayora Zakharovna Saitova Sayora Zakharovna https://www.bustclinica.ru/doctors/saitova-sayora-zaharovna/
Molotov Maxim AleksandrovichPlastic surgeonhttps://www.bustclinica.ru/doctors/molotov-maksim-aleksandrovich/
Molotov Maxim AleksandrovichPlastic surgeonhttps://www.bustclinica.ru/doctors/molotov-maksim-aleksandrovich/
Molotov Maxim AleksandrovichPlastic surgeonhttps://www.bustclinica.ru/doctors/molotov-maksim-aleksandrovich/
Molotov Maxim AleksandrovichPlastic surgeonhttps://www.bustclinica.ru/doctors/molotov-maksim-aleksandrovich/
Molotov Maxim AleksandrovichPlastic surgeonhttps://www.bustclinica.ru/doctors/molotov-maksim-aleksandrovich/
Molotov Maxim AleksandrovichPlastic surgeonhttps://www.bustclinica.ru/doctors/molotov-maksim-aleksandrovich/
Molotov Maxim AleksandrovichPlastic surgeonhttps://www.bustclinica.ru/doctors/molotov-maksim-aleksandrovich/
Molotov Maxim AleksandrovichPlastic surgeonhttps://www.bustclinica.ru/doctors/molotov-maksim-aleksandrovich/
Molotov Maxim AleksandrovichPlastic surgeonhttps://www.bustclinica.ru/doctors/molotov-maksim-aleksandrovich/
Molotov Maxim AleksandrovichPlastic surgeonhttps://www.bustclinica.ru/doctors/molotov-maksim-aleksandrovich/
Zhukova Natalia Vladimirovna Plastic surgeon, maxillofacial surgeon https://www.bustclinica.ru/doctors/zhukova-nataliya-vladimirovna/
Zhukova Natalia Vladimirovna Plastic surgeon, maxillofacial surgeon https://www.bustclinica.ru/doctors/zhukova-nataliya-vladimirovna/
Zhukova Natalia Vladimirovna Plastic surgeon, maxillofacial surgeon https://www.bustclinica.ru/doctors/zhukova-nataliya-vladimirovna/
Zhukova Natalia Vladimirovna Plastic surgeon, maxillofacial surgeon https://www.bustclinica.ru/doctors/zhukova-nataliya-vladimirovna/
Zhukova Natalia Vladimirovna Plastic surgeon, maxillofacial surgeon https://www.bustclinica.ru/doctors/zhukova-nataliya-vladimirovna/
All works can be viewed in the photo gallery
Principle of the technique
Depending on whether the patient plans to breastfeed in the future or not, the plastic surgeon determines the surgical method:
- while maintaining the integrity of the milk ducts;
- with a violation of the integrity of the milk ducts.
Depending on the nature of the defect, the plastic surgeon chooses the type of aesthetic intervention:
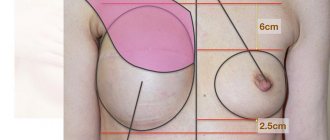
Correction of the size and shape of the areolas.
With an increased diameter of the areolas, manipulation is carried out by eliminating excess tissue.
The areolas receive a new proportional shape. When the areola diameter is reduced, micropigmentation is performed. Elimination of inverted nipple.
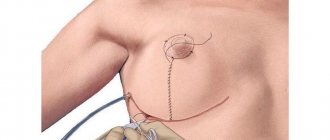
To preserve feeding functions, during the operation a small incision is made in the area of the areola, the fibers that pull the nipple down are separated, the image of the nipple is formed and sutures are applied.
If breastfeeding is not planned, then during the operation the nipple is cut lengthwise to the base, breaking the connection with the milk ducts and connective tissue. To prevent the nipple from going deep into the tissue again, it is fixed at its base with sutures. Reducing the size of the nipples.
If the length is excessive, the upper part of the nipple is excised, and then the surface is sutured.
In this case, the milk ducts are completely blocked. Restoration of the nipple-areolar complex.
The nipple is formed from the skin of the breast, and the areola is created using micropigmentation.
Indications
- inverted nipple;
- nipple hypertrophy;
- asymmetry of nipples and areolas;
- too large (unaesthetic) diameter of the areola;
- cicatricial deformation of the nipple-areolar complex;
- absence of a nipple (congenital or acquired).
You should consult your doctor about contraindications.
Result
- The nipple-areolar complex takes on harmonious size and shape.
- The breasts acquire a natural, aesthetic appearance.
- Psychological complexes are eliminated.
Breast surgery in Siberia
Advantages of correction of the nipple-areolar complex in our Center:
- Each type of operation to correct the nipple-areolar complex has its own proven technique.
- The operations are performed by plastic surgeons with many years of experience, who constantly participate in international conferences and congresses.
- Modern licensed equipment of a high standard.
- High-quality certified medical materials from global manufacturers.
- Author's techniques that allow you to avoid “evidence” from the operation.
- Modern types of anesthesia that reduce side effects and promote comfortable awakening.
- An integrated approach to treatment and rehabilitation, promoting speedy recovery and reducing hospitalization.
- Postoperative wards are classified as “comfort” and are equipped with automated functional beds and a public address system.
Main types of operations
With the help of plastic surgery, you can change the size and shape, eliminate asymmetry, hypertrophy, retraction and other defects of the mammary glands. Surgical correction of the nipples may include:
- reduction or increase in size;
- correction of the pigmented area (areola);
- restoration of a damaged or missing nipple.
Correction of areolas by excision of excess tissue is carried out when the pigmented area is large and irregular in shape. After the operation, the dimensions become proportional. If the nipple is excessively wide, a wedge-shaped excision is performed, and if the nipple is excessively long, the tip or middle part is cut off. To avoid the risk of disruption of breastfeeding, surgery is indicated only for women who are not planning a pregnancy. A new areola is formed using reconstruction. To do this, skin is transplanted from the perineum or tissue from the second breast is taken. Sometimes tattooing with bio-inks can be used. The photo shows the result before and after surgery. Breast areola correction. Plastic surgeon – K. S. Lobachev
After breast removal: how to get back what was lost?
Breast defects are a “sick” topic for women, which they perceive as a real life tragedy. But even in the most difficult cases, which primarily include mastectomy, plastic surgeons can help. In Novosibirsk, the Siberian Institute of Beauty, headed by Professor Olga Borisovna Dobryakova, has been restoring mammary glands and correcting congenital defects for many years.
Women after mastectomy: what next?
Breast cancer ranks first among all cancers in women. Detected in a timely manner, it is now quite successfully treated, but the price of such treatment is most often breast loss. In our country, mastectomy - surgical removal of the mammary gland - is the main method of treating malignant tumors. Moreover, as a rule, surgeons act radically: the gland is completely removed.
So, having defeated cancer, women are faced with another problem that causes them no less torment: how to live with such an aesthetic defect?
Plastic surgeons come to the rescue. They can reconstruct the removed mammary gland, achieving a good visual effect. During the operation, it is possible not only to restore the natural volume, but also to improve the shape of the breast in accordance with all aesthetic canons.
“We perform reconstructive mammoplasty not only after cancer. There are other diagnoses that require aesthetic correction. Underdevelopment of the mammary gland, defects after injuries, pronounced asymmetry of the mammary glands; reconstruction of the mammary glands in transsexuals can be placed in the same category.”
, says Olga Dobryakova, professor, doctor of medical sciences, plastic surgeon, director of the Siberian Institute of Beauty.
All types of plastic surgery are performed at the Siberian Institute of Beauty. Olga Borisovna has performed hundreds of operations to correct defects of the mammary glands. She devoted several hundred scientific articles and textbooks to this topic. The clinic has its own developments, proprietary techniques for performing surgical interventions, which make it possible to recreate the breasts as natural and harmonious as possible.
Breast reconstruction: how shape and volume are created
There are several methods for breast reconstruction. Often, for this purpose, one’s own tissues (autologous tissues) are used - flaps that are transported from different parts of the body. The most common use of the TRAM flap is the transverse rectus abdominis muscle flap. In addition to this, there are flaps from the latissimus dorsi muscle, buttocks, and the lateral surface of the torso. The flaps can be “non-free”, that is, transplanted together with a feeding “pedicle”. Or “free” flaps that are transplanted, and microsurgical work to connect blood vessels takes place in a new place.
Based on my experience, I can say that the visual effect of reconstructing the mammary gland using muscle flaps is good.
Over time, a gradual slight decrease in the gland may occur due to atrophy of muscles and subcutaneous fat, but we initially prevent this by creating a flap that is slightly larger in volume. Olga Dobryakova
The second method is expander dermotension. In the area of the removed mammary gland, tissue deficiency inevitably occurs. In order to restore volume to the breasts, the tissue must first be stretched. This can be done using an expander. This is a “balloon” that is placed in the desired area and is gradually filled with a solution, gently stretching the tissue.
There are several types of expanders. They may differ in type of material and service life. Silicone expanders, according to experts, have good durability, so they are preferable to latex ones, which carry risks of leakage.
In addition, expanders can be permanent or temporary. “Prosthetic expanders” are installed once and do not require replacement with an implant - they are initially filled with silicone gel, the volume of which is replenished by saline solution introduced in stages. A temporary expander is used only to stretch the tissue, and after that it is replaced with a silicone endoprosthesis.
With the help of expander dermodesia, you can achieve the desired volume, beautiful shape, and naturalness of the mammary glands. However, this is not always easy. If you plan the operation incorrectly, you can get the effect of a bump, which will look very unaesthetic on the body. In particular, this happens when the doctor opts for a small expander and is in too much of a hurry to complete the work.
“How to get the desired result? I take a large expander and stretch the tissue very slowly over a long period of time. It may take six months or a year for a mammary gland to form with a clear submammary fold. This is the only way the breasts will end up looking like real ones.”
, - Dobryakova shares his professional secrets.
The author's developments include the introduction of botulinum toxin before stretching. Reacting to the injections, the tissues relax and stretching occurs more effectively.
Patient, slow stretching of tissues using an expander can increase their volume tens of times. This allows the surgeon to form a mammary gland that is as close to natural as possible.
Sometimes breast reconstruction requires a combination of both methods - placing a flap and then stretching the tissue with an expander. For example, if a patient has ulcerative defects, they must first be covered with a flap, and then work on the volume.
The second gland may also require correction. If it is irregularly shaped, or has severe ptosis, it also needs to be brought into shape, sometimes with the help of an implant. This is how the doctor achieves symmetry of the mammary glands and recreates the overall aesthetics of the female breast.
The artistic element is very important in reconstructive mammoplasty. Just “making breasts” is not difficult. And making natural breasts is a creative process that requires effort and special skills of a plastic surgeon.
Nipple-areolar complex: methods of restoration
After the volume and shape of the gland has been created, it is necessary to reconstruct the nipple-areolar complex. There are several ways to restore it.
To recreate the areola, today a technique is used to transplant pigmented skin from different areas of the body: from the inner surface of the upper thigh, labia. If possible, the second areola can also become a “donor”. Plastic surgeons identify these methods as the main ones, and alternative methods include creating an areola using a tattoo, for example.
“Skin grafting taken from the upper part of the inner thigh gives a good aesthetic effect and the healing of such flaps usually occurs without problems. In addition, this method can be considered the most reliable and psychologically comfortable for patients.”
,” Olga Borisovna shares her observations.
After recreating the areola, surgeons are faced with another task - it is necessary to form a nipple on it. Various techniques are also used for this. For example, there are known methods for cutting out the nipple protrusion using flaps in the center of the areola.
At the Siberian Institute of Beauty, the author’s technique, developed in 2010 by professors O.B., is used to recreate the nipple. Dobryakova, B.S. Dobryakov. It consists of using an implant – a silicone ball.
The Siberian Institute of Beauty has more than a dozen inventions that have opened up new possibilities for aesthetic surgery. Reconstructing the nipple using a silicone ball is an original technique that has improved the results of reconstructive mammoplasty.
At the first stage, a silicone ball is inserted into the donor site, which is most often located in the upper part of the inner thigh. Within 1-2 months it remains under the skin, growing into a strong connective tissue capsule. It is then removed and placed in the center of the areola, forming the nipple.
The goal of reconstructive mammoplasty is to make the breasts look beautiful and natural. Moreover, not only in underwear, but also without it. If a woman who has undergone surgery (and sometimes more than one) still cannot afford to undress, it means that the reconstruction was pointless, and time, money and nerves were wasted.
“I consider such breast reconstructions to be a special merit when, after restoration, the mammary glands become so natural and harmonious that they look even better than before the oncological operation.”
, says Professor Dobryakova.
“I have never had such beautiful breasts as now, I feel not just a full-fledged person, but also a desirable woman, I am happier than ever,” this patient’s review is the highest assessment of my work.
Olga Dobryakova
Siberian Beauty Institute:
2-910-946, outpatient clinic: Novosibirsk, st. Novaya Zarya, 17 A; hospital: Novosibirsk, st. Zalesskogo, 6, building 9, 7th floor, room. 737; www.dobryakova.ru
https://m.vk.com/olga.dobryakova
https://www.imgrum.org/user/sib.institutkrasoty/3283685133
https://www.instagram.com/sib.institutkrasoty/
There are contraindications. Specialist consultation is required.
Preparing for surgery
Since nipple correction is a surgical procedure, the patient must undergo a preliminary examination. As part of the preparation, ultrasound, ECG, mammography are performed, and the necessary tests are taken. A couple of weeks before the scheduled date, you should stop taking medications, especially those that affect blood clotting. It is also necessary to refrain from smoking and drinking alcohol. The photo shows the result before and after surgery. Breast areola correction. Plastic surgeon – K. S. Lobachev
Breast reconstruction with silicone implants
This type of reconstructive surgery is the most popular in the world and is used in more than 80% of women who undergo breast reconstruction.
This popularity is due to the fact that this method is the least traumatic, does not create additional scars and has a fairly short recovery period.
Figure 1. The first stage of reconstruction - using an expander
Most often, this reconstruction method includes two main stages. In the first, a tissue expander is placed under the skin and muscle tissue of the chest wall, which is an “empty” silicone implant with a magnetic port that allows it to be filled with sterile saline (see Figure 1). Filling and stretching the expander allows you to stretch the soft tissue and create the volume and shape of the future mammary gland. Tissue expanders can be of various shapes and sizes, which allows you to choose the optimal one, taking into account individual characteristics.
“Pumping up” of the expander after implantation is carried out once every two or three weeks on an outpatient basis. This is an absolutely safe and painless procedure that allows you to gradually increase the expander volume. The process of filling the expander takes from two to five months, depending on its volume and tissue stretch.
At the second stage, the expander is replaced with a permanent silicone implant, the shape and volume of which is also selected individually. At this stage, the final shape of the reconstructed breast is usually created, and the opposite one is often corrected in order to improve its appearance and give the area a symmetrical appearance. Surgeries on the opposite gland are safe; they cannot provoke tumor growth, but only help to harmonize the external appearance of the body (see photos 1-7).
Photo 1. Before and after breast reconstruction with silicone implants. Patient 1
Photo 2. Before and after breast reconstruction with silicone implants. Patient 1
Photo 3. Before and after breast reconstruction with silicone implants. Patient 1
Photo 4. Before and after breast reconstruction with silicone implants. Patient 2
Photo 5. Before and after breast reconstruction with silicone implants. Patient 2
Photo 6. Before and after breast reconstruction with silicone implants. Patient 3
Photo 7. Before and after breast reconstruction with silicone implants. Patient 3
Figure 2. Single-stage breast reconstruction. Scheme
With one-stage reconstructions, in some cases it is possible to do without the expander stretching stage. In these cases, a permanent silicone implant is immediately placed after the mastectomy.
Such operations usually require the use of additional materials to stabilize the position of the implant (see Figure 2), the cost of which can be quite significant. However, in some cases, especially when it comes to bilateral operations, this approach may be the optimal choice (see photos 8-10).
Photo 8. Result of one-stage breast reconstruction
Photo 9. Result of one-stage breast reconstruction
Photo 10. Result of one-stage breast reconstruction
How is the nipple-areolar complex corrected?
The operation on the nipples and areolas lasts about one hour, so it can be performed under both general anesthesia and local anesthesia. There are three main directions in which correction is carried out:
- changing the position of the nipples and correcting their size;
- enlargement or reduction of nipples in combination with giving the correct shape to the areolas;
- restoration of the entire nipple-areolar complex.
You can find out the exact price for nipple correction in each specific case only after consulting a doctor. If you have any questions, please contact our managers for telephone consultation. You can make an appointment with specialists through the online form.
Nipple and areola reconstruction
One of the most frequently asked questions on the topic of breast reconstruction is how to create the nipple-areolar complex? Without a doubt, the nipple and areola are an important part of the mammary gland, the most “erotic”, and therefore public display of this area is considered indecent, and images on social networks are subject to deletion.
That is why I bring to your attention a short overview of modern methods of reconstruction of the nipple and areola during reconstruction of the breast removed after mastectomy.
Of course, the priority is to preserve the nipple and areola, even if a mastectomy is necessary. Nipple and areola sparing mastectomy or subcutaneous mastectomy are now increasingly performed in our practice due to the early detection of malignant tumors.
However, the proximity of the tumor to the central zone or large tumors force us to perform a mastectomy with removal of the nipple and areola. This need is due to the anatomy of the mammary gland. In the area of the nipple and areola there is no layer of subcutaneous fat and the breast tissue is directly connected to the skin. Therefore, preserving the nipple-areolar complex means leaving some tissue directly in this place.
To avoid leaving part of the tumor in this area, a biopsy is performed during surgery from the submamillary area and, if signs of a tumor are detected, the nipple and areola are removed.
In this case, after restoring the shape and volume of the mammary gland, in most cases the question arises of recreating the missing nipple and areola. I recommend performing this procedure no earlier than 3-4 months after the main stage of reconstruction. This is due to the fact that the final position of the mammary glands after reconstruction and correction of the opposite one is formed no earlier than this period, and the position of the future nipple-areolar complex can be more accurately determined. The procedure is performed on an outpatient basis, under local anesthesia and does not require a large number of tests.
Before reconstructing the nipple, the patient and I select the optimal method in terms of results and make markings.
To do this, the optimal position of the future nipple relative to the reconstructed gland and the location of the opposite nipple is determined. These points do not always coincide, because it is not always possible to achieve perfect symmetry, so I determine the optimal point, take a photograph and discuss the position of the future nipple with the patient. If necessary, we make adjustments to the position where the nipple should be located.
There are currently two main approaches to nipple reconstruction.
The first is using local fabrics. To do this, local flaps are mobilized, from which a column of skin is formed, simulating a nipple.
The most popular method in my practice is the CV flap and its modifications, but there are other flaps.
In my opinion, this method is more promising from the point of view of obtaining a long-term stable result when reconstructing the breast with one’s own tissue - a flap on the latissimus dorsi muscle (LDL) or from the lower abdomen (TRAM or DIEP).
When using this technique after reconstruction with an implant due to tissue tension, the nipple created using local tissues may eventually lose its projection and become flat.
To prevent this and stabilize the result, high-density hyaluronic acid preparations can be administered.
Another, no less promising method is donor tissue transplantation . These tissues may be part of the opposite nipple or labia minora.
The labia minora is rarely used, but this method should be kept in reserve in combination with or without aesthetic intimate plastic surgery when, for example, both nipples have been removed and reconstruction using local flaps has not been successful enough.
The most effective technique in my practice is to transplant part of the opposite nipple. This is the most reliable method that brings stable, aesthetically valuable results. The only limitation is the small nipple of the opposite breast. In this case, local flap techniques are quite capable of coping with the task of reconstruction.
If the donor nipple is of sufficient size, then dividing it in a vertical or horizontal plane is not technically difficult. The graft is transferred to a previously prepared site in the area of the future nipple position and sutured. Several stitches are also placed on the donor nipple.
The opposite breast is enlarged with an implant, and half of the nipple is transplanted onto the reconstructed breast
This method results in two nipples that are almost identical in size and structure.
To obtain the “full” restoration effect, it is also necessary to create an areola. Previously, various skin flaps were used to create an areola, which were transplanted from the area of the opposite areola during mastopexy (lift), when excess skin was excised. Another donor site was the inguinal crease area. In this area, the skin has darker pigment and can therefore mimic the pigmentation of the areola.
Today, most areolas are created by intradermal pigmentation in the process of permanent tattooing. The selection of pigment and procedure is carried out by a specialist in this field. To achieve a good result, it is advisable to perform this procedure on both sides.
Due to the fact that the results of breast reconstruction are now approaching aesthetic surgeries, reconstruction of the nipple and areola is an extremely popular procedure and is performed on almost every patient undergoing reconstructive surgery.
It is also important to understand that to achieve the optimal result of reconstruction of the nipple and areola, sometimes several stages are necessary and the participation of at least two specialists - a plastic surgeon and a cosmetologist.
Author of the article: Sergey Malygin, 04/04/2018
Execution technique
Reducing the size of the nipple can be done in two ways:
- sectoral resection involves cutting out a triangle-shaped area and then suturing the edges;
- excision with a wedge involves reducing the size due to the apex, while also cutting part of the milk ducts.
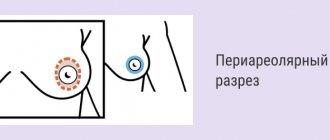
An inverted nipple is corrected by moving it to its normal position after cutting the cords that hold it in place. It is also possible to create a support in various ways. The effect after surgery and the aesthetics of the result depend not only on the professionalism of the doctors, but also on the patient’s compliance with the regimen.
Contraindications for surgery
The operation can only be hampered by the patient’s general surgical limitations:
- oncology;
- benign changes in the breast;
- exacerbation of chronic diseases;
- severe systemic pathologies;
- changes in the blood coagulation system;
- pregnancy or lactation.
In order for the correction to be successful, you need to wait 12 months after breastfeeding. Also, the operation is not performed on persons under 18 years of age, since breast formation has not yet been completed until this age.
Side effects
If the doctor's recommendations are not followed, complications may arise:
- Hematomas are normally small in size and disappear on their own within 5–7 days. If the bruises hurt and tend to increase, the shape of the mammary glands changes, you need to contact a medical facility. This may be a symptom of subcutaneous bleeding.
- Changes in the sensitivity of the nipples and areolas often occur due to the dissection of nerve fibers. Disturbance of innervation can persist from several months to a year.
- Inflammation of the soft tissues is accompanied by leakage of serous fluid in the area of the sutures, redness of the skin, and suppuration. Body temperature may rise.
- The formation of hypertrophic scars as a result of improper breast care, allergies to suture material, and excessive physical activity.
- Microcracks on the nipples and areolas with thin and sensitive skin.
Breast reconstruction: what do women fear most?
Removal of the mammary glands (mastectomy) is carried out under the influence of various factors. The most common cause is breast cancer. Every year this disease is diagnosed in tens of thousands of women. Partial or complete removal of the breast becomes the main part of the treatment of the tumor process and saves the lives of many patients. However, after prolonged therapy, women are left alone with a huge complex - the absence of breasts. In this case, reconstructive breast surgery is recommended, the purpose of which is to restore the previous aesthetically attractive forms. What are the pros and cons of breast reconstruction and why are women so afraid of the consequences of surgery? Let us examine the main issues of this topic, based on the opinion of the leading plastic surgeon at Frau Klinik, Sergei Nikolaevich Blokhin.
The mammary glands not only perform the function of feeding, they also form the normal proportions of the female body. The need to perform a mastectomy, in addition to cancer, is due to various mammological diseases: purulent mastitis, fibroadenomatosis, numerous cysts, etc. Breast reconstruction after mastectomy involves restoring the lost mammary gland using implants, your own tissue, or a combination of two techniques. Let's look at the main points that make many patients doubt about breast reconstruction.
Most often, mastectomy is preceded by breast cancer; in this case, reconstructive mammoplasty will help to recreate lost beauty and overcome complexes.
Unaesthetic result
After breast reconstruction, scars inevitably remain on the breasts, which spoil its aesthetic appearance. But this is not a cause for concern - after 6-12 months, the redness and bumpiness will subside, and the scars will become less noticeable. Also, the problem of aesthetics lies in the restoration of the areola and nipple, since breast reconstruction cannot be considered complete without restoration of the nipple-areolar complex.
There are a lot of methods for reconstructing the nipple and areola, but most often it is carried out using the transplantation of the patient’s own tissue or using tattooing. Simultaneously with plastic surgery of the nipple-areolar complex, correction of the formed mammary gland, and sometimes healthy breasts, is usually performed in order to recreate the correct and harmonious proportions of the body.
Consequences of installing implants
Swelling and pain when performing movements often accompany the rehabilitation period after surgery. An elastic bandage or support bra will help minimize swelling and support the reconstructed breasts. Women are also afraid that the implant may lose its shape or move to the side, which will affect the appearance of the breast. But today, plastic surgery clinics use only the highest quality implants, which guarantee a natural and aesthetic appearance of the breast, and the barrier layer of the implant prevents the leakage of the gel, even if it is damaged, which reduces the likelihood of implant displacement to zero.
Loss of sensation is another negative consequence of reconstructive surgery. But do not forget that the main task of the operation, first of all, is to restore the shape and volume, as well as the consistency of the mammary gland. Sensitivity in this case is impaired in almost any outcome.
Asymmetry
If only one breast was affected by the mastectomy, then the operation is performed only on it. But there are also cases when a lift, reduction or enlargement of the opposite breast is required to improve the symmetry, size and position of both mammary glands.
When performing breast reconstruction, everything possible is done to eliminate breast asymmetry
Using your own fabrics
If there is not enough soft tissue in the area of the removed mammary gland, the operation is performed using one’s own tissue. In this case, using a TRAM flap (transverse rectus abdominis muscle flap).
The choice of method depends on many factors: excess or lack of tissue, where and how much skin can be preserved, the condition of the second mammary gland - after all, it is necessary to achieve maximum symmetry, and in half of the cases corrective surgery has to be done on the other side. After this technique, as a result of borrowing a skin flap from the abdomen, a scar will form in this area, but just as in the case of scars remaining on the chest after reconstruction, they will all disappear within a year, leaving behind only a barely noticeable mark surgical intervention.
Sergey Blokhin comments:
Professor, Doctor of Medical Sciences, famous Russian plastic and reconstructive surgeon, head of the Frau Klinik
Reconstruction with the patient’s own tissue is a priori a more complex intervention than breast reconstruction with an implant. The choice of reconstruction technique depends, first of all, on the amount of tissue on the removed breast: it is important to realize that the implant must be inserted somewhere, and when this place is completely missing, the breast must be formed using the patient’s own tissue - a TRAM flap.
Long rehabilitation period
The operation is a fairly complex intervention, so the rehabilitation period lasts much longer - on average from six months to a year. Despite this, the result of the reconstruction can be assessed after three months. You will have to check with your doctor regularly for several months after the reconstruction. In addition to a monthly check-up with a surgeon, do not forget about a mammogram, which is mandatory for all women. Also, during the rehabilitation period, it is necessary to follow all the surgeon’s recommendations, because breast reconstruction is one of the most difficult operations.
There are a number of general rules, which include the following points:
- it is necessary to avoid heavy lifting, as well as any physical (including sports) activities for about 6 months after surgery;
- you should “keep” your weight normal to avoid changes in the appearance of the breasts;
- any diet, lack of vitamins contained in meat, fish, vegetables, fruits can aggravate your condition in the postoperative period;
- smoking negatively affects the healing process, so it is better to abstain from it during the rehabilitation period; drinking alcohol is also prohibited;
- It is prohibited to take drugs that affect blood clotting (including aspirin);
- You should wear a special bandage for about six months.
More detailed information about breast reconstruction can be obtained during a consultation with a specialist at the Frau Klinik plastic surgery clinic. Make an appointment by phone.