Lipofilling for breast augmentation. About the result and breast cancer.
Anton Zakharov: Breast cancer is one of the most common diseases in the structure of cancer incidence in general. The fat transplanted into the mammary gland does not take root completely. And now the most interesting thing that the advertisement is silent about.
Anton Zakharov: Greetings. Today we will discuss such a relevant, extremely pressing topic for today as lipofilling of the mammary gland.
It's no secret that many of our patients want to change the shape and volume of their mammary glands. Previously, this problem was solved with the help of implants. But today, the technology of transplanting one’s own fat from places where for some reason it is not needed or is removed, into the structure of the mammary gland to create shape and volume is being actively introduced into the market, and the doctors who are involved in this are introducing it into the minds of patients.
The technology is presented in the information field as innovative, solving all the main problems, allowing not to install breast implants and having a shorter rehabilitation, comfortable recovery. Some advantages.
How is the situation really?
The first step is the collection of fatty tissue. Most often, some donor area is selected for liposuction, for example, it can be the lateral parts of the lower back or the front surface of the abdomen - where there are obvious excesses that the patient wants to get rid of.
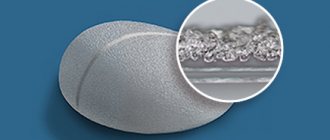
This fatty tissue is collected with special low-pressure cannulas in order to maintain maximum integrity of the transplanted material. Next, one or another treatment is carried out, depending on the technology used, of the harvested graft. And at the final stage, the transplanted tissue is introduced through thin punctures with cannulas to form the shape of the mammary gland and, first of all, its volume. In general, the concept of this manipulation is exactly this.
It is often declared that this technique makes it possible to fill the volume of the mammary gland and solve the problem of unaesthetic contours.
In reality, simple mathematics works. The fact is that fat that is transplanted from one zone (donor) to another (that is, recipient) does not take root completely. According to all world studies, fat shrinkage, that is, the residual volume that will exist in tissues for a long time, is at least 50%. That is, in order to get a 50 milliliter increase in volume, you need to transplant at least 100.
The fact is that there are certain restrictions on fat transplantation to a specific anatomical area. It is believed that it is not recommended to transplant more than 100-150 milliliters into one zone at a time, because this can lead to a number of complications associated with a lack of blood supply in a given zone for the transplanted tissue, and worsens the survival rate.
Now let's do some simple calculations. That is, in order to obtain a volume increase of 300 milliliters (this is the average volume of an implant that is placed to enlarge the mammary gland), we need to transplant a total of about 600 milliliters of fat, which, accordingly, will then turn into these 300.
At the same time, understanding that 100-150 milliliters can be transplanted at a time, it becomes clear that in order to compensate for the volume deficit of 300, we need 5-6 operations.
This is delicately kept silent in the advertising.
That is, while this operation is presented externally as extremely effective and efficient, what remains behind the scenes is that it is not possible to immediately solve the significant problem of volume deficiency, which our patients most often address.
Second important aspect. Fat transferred into the mammary gland does not provide effective support for the breast. That is, if a patient has implants installed, this not only gives volume. This also dictates the shape, that is, it allows us to build the structure of the mammary gland the way we want to see it. When transplanting fat, these tissues do not perform any scaffolding function. Accordingly, we cannot effectively control the shape of the breast, especially when it comes to long-term results.
And now the most interesting thing that the advertisement is silent about. It's no secret that breast cancer is one of the most common diseases in the structure of cancer incidence in general. And every woman after 40 years of age should undergo a routine screening examination in order to determine the development of this disease in the early stages, if it does occur. And, accordingly, receive effective treatment.
You need to understand that even a one-time lipofilling of the mammary glands forever makes all methods of X-ray diagnostics of this organ ineffective, since the fat that is introduced into the gland and surrounding structure during lipofilling creates certain X-ray shadows, and studies of the mammary gland using mammography, computer tomography or magnetic resonance imaging are no longer considered informative. That is, an effective screening examination to assess one’s cancer status is no longer possible. And this, of course, when promoting these manipulations, is delicately kept silent or forgotten to be said.
But it seems to me that this is fundamentally significant information for a woman’s future life, because if X-ray methods for assessing cancer status are no longer effective, then after 40 years a person will have to donate blood for tumor markers every two months for life in order to be safe and not miss such a serious disease of the mammary gland.
Of course, in this case we are talking about aggressive, volumetric lipofilling used to enlarge the mammary gland.
But also in the practice of a plastic surgeon, there is so-called camouflage, when extremely small volumes of transplanted fat are used to camouflage, respectively, some delicate surface defects along the implant. It's not the same thing. Camouflage does not interfere with the structure of the mammary gland, and it is performed in an extremely small volume, so similar effects that we are talking about do not develop in this case.
Breast reconstruction
Photo report 1.
Before
7 days after stage 3 of reconstruction
Patient after radical mastectomy 3 years later (convalescent).
At the moment, a three-stage reconstruction of the right breast and a T-shaped lift of the left breast have been performed.
Stage 1.
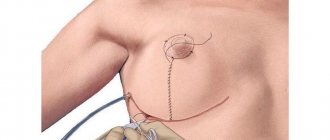
Installation of a subcutaneous expander and three-month stretching of the skin and scars of the right breast.
Marking before surgery.
Template for correct installation of the expander.
Installation of an expander through an incision after oncological surgery.
The expander is installed.
The expander has reached the required volume and will be replaced with an implant.
Stage 2.
Removal of the expander and installation of a 390 ml anatomical implant in the left breast.
Removing the expander.
The expander has been removed.
View of the expander after removal along with the anterior layer of the capsule.
Stage 3.
T-shaped lift of the left breast and reconstruction of the areola and creation of a neo-nipple of the right breast from the tissue of the left breast obtained during the lift.
View of the reconstructed breast after implant installation after 8 months.
Reconstruction of the nipple-areola complex of the reconstructed breast using tissue obtained from a healthy breast after a lift.
Stage 4 is planned: subcutaneous autolipotransplantation (lipofilling) of the right (reconstructed) breast and liposuction of the waist.
Multi-stage reconstruction allows each operation to be performed with high precision and control of the result, since the mammary glands are a paired organ and it is important to make them as identical as possible, provided that the tissues and nipple-areolar complex of one breast are completely absent. In addition, there are risks of suture failure or rejection of the transplanted areola and the reconstructed nipple.
Future stages of lipofilling will make it possible to increase the volume of the integumentary tissue of the reconstructed gland and restore the softness of the breast.
To plan all stages and select an implant, the VECTRA-3M 3D modeling system was used. This is very important for the doctor (even a very experienced one) and the patient. Nothing will work out by eye. Visualization of each stage gives a woman inspiration and patience, especially after suffering from an illness, and even at such a young age.
Photo report 2.
The patient has already undergone 2 stages in another clinic.
Stage 1.
Removal of the mammary gland.
Stage 2.
Installation of an expander for tissue stretching.
We will go through all other stages with the patient together.
Stage 3.
Removal of the expander and installation of a permanent implant.
Stage 4.
Lifting one breast and restoring the areola on the right breast using tissue from the left areola.
Stage 3. Removal of the expander and installation of a permanent implant.
Breast appearance before surgery:
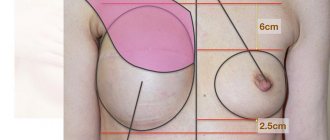
As a result of the installation of the expander and its swing, the inframammary fold was displaced and the fold of the right breast is located significantly lower than the left healthy breast. We will remove the expander and install a permanent implant, restore the submammary fold of the right gland, expand the breast pocket upward to raise the right breast to the level of the left breast, and excise scars and adhesions. As a result of the operation, the submammary folds of the right and left breasts will be at the same level.
Photo of the breast with an expander:
Carrying out the necessary measurements to plan the tactics of the operation:
An incision is made through which the expander will be removed and the implant installed:
Removing the expander:
Expander removal video.
Remote expander view:
Restoration of the submammary fold, expansion of the breast pocket, dissection of scars and adhesions:
Implant installation:
Skin suture after implant placement:
Video commentary by Sviridov S.V. after the operation is completed:
View of the breast before surgery and immediately after:
Before
After
View of the breast the day after surgery:
Video before surgery:
Video after surgery:
Photos before and after surgery:
Before
After
An anatomically shaped 350 ml implant was installed.
Disadvantages of breast augmentation through the areola
- With a small diameter of the areolas, the patient is limited in choosing the size of implants.
- There is an increased risk of damage to nerve endings and milk ducts, which can negatively affect a woman's ability to lactate. This does not mean that after breast augmentation through the areola, the patient will lose the ability to breastfeed. According to statistics, 7% of women experience difficulties with milk production during pregnancy, which is only in isolated cases associated with mammoplasty. Doctors at the Pirogov Clinic have successfully performed more than 10,000 thousand plastic surgeries since 1999. By contacting us, you can be sure that at all stages of the operation, from examination to completion of rehabilitation, you will receive medical care based on high professionalism and sensitive attention to your health.