Diastasis of the rectus abdominis muscles is the separation of the inner edges of these muscles due to weakening and stretching of the linea alba.
Women often complain about this defect in the period after the birth of a child, since during pregnancy the pressure on the anterior wall of the abdomen increases and the muscles of the white line “diverge,” but excessive physical activity, obesity and hereditary predisposition can also be the causes.
Some people try to remove diastasis with special exercises, but it is important to understand that the deformation of the connective tissue cannot be corrected by training. Exercises strengthen the muscles, but they have no effect on reducing the distance between them. Suturing the diastasis is the only possible way to eliminate the defect.
Fortunately, the operation to correct diastasis, performed by specialists at our clinic, is low-traumatic and is characterized by the absence of incisions and unsightly scars after the intervention.
The peculiarity of my approach to performing diastasis correction using minimally invasive techniques
There is no single way to correct abdominal diastasis, just as there are no similar women. In each specific case, everything is decided individually, based on the stage of the disease, associated cosmetic problems and the wishes of the patient.
The choice of surgical intervention method for diastasis depends on the stage of the disease, the presence or absence of ptosis (drooping) of the skin and unsightly scars on the anterior abdominal wall.
I perform a whole range of proprietary minimally invasive procedures
interventions at various stages of the disease:
Stage 1 – transumbilical plastic surgery of diastasis using a mesh endoprosthesis (with a diastasis length of 4-6 cm) or laparoscopic plastic surgery of diastasis using a mesh intraperitoneal endoprosthesis (with a diastasis length of 6-18 cm);
Stages 2 and 3 – laparoscopic diastasis repair using thread suturing with a long resorption period using or without a mesh intraperitoneal endoprosthesis;
Stages 1,2,3, in the presence of abdominal ptosis or unsightly scars on the anterior abdominal wall - abdominoplasty in combination with diastasis plastic surgery and the use of a mesh endoprosthesis.
At any stage of the disease and the presence of concomitant ventral hernias, their simultaneous correction is always performed.
If there are concomitant diseases of the abdominal and pelvic organs (gastrointestinal tract disease, ovarian cyst, etc.), if the patient wishes, these problems can also be eliminated using laparoscopic access.
All operations can be divided according to the type of access to the midline and the type of reconstruction of the abdominal wall itself. A reasonable combination of access and type of intervention gives an excellent result of the operation.
All operations are performed under general anesthesia.
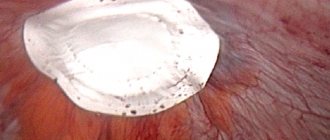
Rice. 1. Transumbilical plastic surgery of diastasis with mesh endoprosthesis
Rice. 2. Classical open plastic surgery of diastasis with local tissues without a mesh implant (incision 12-14 cm).
Rice. 3. Option of laparoscopic diastasis repair using a mesh intraperitoneal endoprosthesis
Rice. 4. Option of laparoscopic diastasis repair using a mesh intraperitoneal endoprosthesis
Rice. 5. Abdominoplasty in combination with diastasis plastic surgery and the use of a mesh endoprosthesis.
Patent. Method of Lipoabdominoplasty with navel relocation
Treatment methods
- Conservative treatment (for degrees 1-2 of diastasis) consists of performing special physical exercises, breathing exercises, avoiding heavy lifting and following a diet. In this case, we can expect some reduction in aesthetic defects. If there is a root cause of the disease, then its treatment is imperative.
- Surgical treatment is indicated for grade 3 diastasis. The presence of a concomitant hernia is an additional indication for surgery, and usually surgery in this case is the only treatment option and allows you to get rid of two problems at the same time.
Transumbilical plastic surgery of diastasis with mesh endoprosthesis
I use this type of operation for stage 1 diastasis.
The essence of the technique is as follows. On the skin of the abdomen, around the navel, I make a cosmetic incision - a mini access of 3-4 cm. Next, under endoscopic control, I separate the aponeurosis along the edge of the diastasis at a distance of 10-16 cm (depending on the size of the defect). Then I open the sheath of the rectus muscles on both sides and place a mesh implant in their bed (Fig. 1). I fix the endoprosthesis around the perimeter with a non-absorbable thread “Prolene 2-0” on an atraumatic needle. Thus, the implant is located in the bed of the rectus abdominis muscles, and the abdominal organs are protected by the wall of the rectus sheath and the peritoneum. In front, above the mesh, there is a layer of muscle, aponeurosis, subcutaneous tissue and skin. Therefore, patients do not feel the implant; after germination with its own connective tissue, it becomes a second native aponeurosis. At the next stage, I perform suturing of the aponeurosis and elimination of diastasis (the rectus abdominis muscles come closer together - this leads to their good function and cosmetic effect). The wound must be closed with an intradermal cosmetic suture. For comparison, the view of the abdominal wall is shown when a classic open diastasis is performed with local plastic tissue (Fig. 2) without a mesh implant (incision 12-14 cm).
Abdominoplasty in combination with diastasis plastic surgery and the use of a mesh endoprosthesis.
I use this type of operation for all stages of the disease, in the presence of abdominal ptosis or unsightly scars on the anterior abdominal wall.
The essence of the technique is as follows. Depending on the severity of soft tissue ptosis and the thickness of the subcutaneous fat layer of the abdominal wall, the presence of rough and unsightly scars on the anterior abdominal wall, one or another type of abdominoplasty is performed. During abdominoplasty, the sheath of the rectus muscles is opened on both sides and a mesh implant is placed in their bed, which is fixed around the perimeter with a non-absorbable thread “Prolene 2-0” on an atraumatic needle (Fig. 5). Next, the aponeurosis is sutured and the diastasis is eliminated. At the same time, the rectus abdominis muscles come closer together, which leads to their good function and cosmetic effect. At the final stage, the wound after abdominoplasty is closed and the subcutaneous tissue is drained.
Possible reasons for the development of pathology
The most common cause of diastasis is increased pressure in the abdominal area. Factors that cause an increase in blood pressure levels can be different, for example:
- loss of elasticity of muscle structures as a result of rapid weight loss;
- excessively heavy physical activity;
- dysplasia - errors in the formation of tissues and organs. In addition to muscle divergence, phenomena such as hernia, varicose veins, hemorrhoids, and so on may also occur;
- pregnancy. Due to changes in hormonal levels, collagen formation decreases, tissues lose elasticity and become loose. At the same time, the uterus increases in size, putting more pressure on weakened muscles and the linea alba.
In 60% of cases, muscle discrepancy in women occurs during pregnancy. This phenomenon manifests itself in the middle of the 2nd trimester - during this period the muscles move apart due to increasing pressure. In a normal case, the uterus should return to its original size after childbirth, and the width of the white line should shrink to 2 cm.
But in many cases, during rehabilitation there are aggravating factors due to which the tissues cannot return to their original position on their own. Such nuances could be:
- mature age of a new mother;
- obesity before and during pregnancy;
- the fruit is too big;
- many pregnancies and births in the past;
- several fetuses during one pregnancy;
- complications during pregnancy;
- returning to sports too soon after the birth of a child.
Diastasis can also develop in children, most often in premature babies. The main reason for the development of muscle discrepancies in children is the baby’s weak muscles and tendons. Often the problem disappears on its own during the first year of a child’s life. At this time, the muscles are just gaining tone, and the ligaments are getting stronger. The risk that diastasis will persist is mainly in babies with Down syndrome.
Only in 1.5% of all cases, diastasis is found in males. The main reasons for the development of this pathology in men are the same as in women:
- excess weight;
- dysplasia;
- fast weight loss.
Excessive physical activity can also provoke diastasis (as well as hernias and varicose veins) in men.
Main signs of diastasis
For a long period of time, diastasis is asymptomatic. The manifestations of this pathology increase as muscle separation develops and complications arise. In female representatives, the peak manifestation of symptoms of muscle separation occurs in the period after pregnancy and childbirth, and in male patients - when diastasis is already in a serious condition.
The main and most obvious sign of diastasis is a rounded bulge along the abdomen. When the press is deliberately stressed, a groove appears between the two parts of the body. In men, even with serious loads during abdominal exercises, it does not acquire the desired relief.
If diastasis progresses, structural features of muscle tissue and disturbances in muscle functioning can cause more serious phenomena, for example:
- pain in the back, lower back;
- postural deformation;
- rapid fatigue;
- Gastrointestinal dysfunction with heartburn, belching, stomach pain, stool disorders, increased gas formation.
With third degree diastasis, dangerous complications can develop such as:
- ptosis, organ prolapse;
- intestinal obstruction;
- urinary incontinence;
- feeling of tiredness in the legs when walking;
- muscle atrophy in the abdominal area.
Medical methods for detecting diastasis
The manifestation of any of the above symptoms, as well as the presence of a predisposition (recent childbirth or severe physical activity) is a reason to come for examination to a specialist. You should not delay visiting a doctor; you should come to the appointment as soon as possible, instead of delaying and waiting for serious complications.
Most people have no idea which doctor identifies the presence of abdominal muscle discrepancies. The help of a plastic surgeon directly is needed: an experienced doctor will be able to identify the presence of diastasis through just palpation.
During the examination, the person lies on his back, with his legs slightly bent and his feet resting on the couch. The specialist says to tighten your abs, raising your shoulder blades and head a little at the same time. He palpates the abdomen, measures the distance of divergence, and identifies the presence and degree of diastasis. At the same time, grade 3 diastasis is obvious even without palpation and standing.
Sometimes determining the width of the white line is difficult due to excess weight. For such people, the surgeon prescribes an ultrasound. The same study is prescribed if there are hints of a complication: hernia or displacement of organs. In some cases, x-rays and/or tomography may be required.
Self-diagnosis of diastasis
Muscle expansion can be detected independently. This can be done through a simple test, whereby the distance between the edges of the rectus muscle is measured. To perform self-diagnosis, you need to perform the following steps.
- Lie on your back on a hard surface with your knees bent
- Place one hand under your head, place the other on the white line, slightly above the navel.
- Relax your body and lift your chest
- Using your fingertips, feel the discrepancy between the muscles; The gap is best felt between the navel and the xiphoid. shoot
- If the diastasis exceeds 2 fingers in width, you should consult a surgeon as soon as possible
This technique is as similar as possible to the professional approach to diagnosis used by surgeons. This is the easiest method for identifying diastasis without the participation of a doctor and a professional examination.
How to eliminate diastasis?
The method of getting rid of diastasis is selected depending on the degree of development of the pathology and the nature of its manifestation. At the first stage, you just need to follow the doctor’s recommendations to strengthen the abdominal muscles and reduce the discrepancy:
- losing weight to normal weight;
- adherence to the principles of a healthy diet with reduced consumption of fatty, sweet, etc.;
- taking daily water intake;
- wearing a bandage that supports the abdomen;
- massage and similar physiotherapy procedures;
- yoga, swimming, Pilates, exercise therapy and other suitable sports.
Exercise therapy should be carried out by an appropriate specialist who will draw up a program and select a load taking into account the condition of the patient’s body. Much attention should be paid to the deep transverse and oblique muscles, which reduce the degree of divergence of the white line at a certain level of tone.
Exercise therapy is useful even for pregnant women. A set of special procedures will help prevent the formation of pathology and reduce the duration of rehabilitation of the body after the birth of a child.
The set of exercises for diastasis does not include those that strain the abs. You should also not perform exercises while standing, including resting on your knees and elbows. Such loads are allowed only after restoration of the original width of the lumen has been completed.
With a more advanced degree of discrepancy, it will no longer be possible to remove diastasis through physical activity and massage. In this case, the problem can be eliminated only through surgery, which will put the muscle corset in the right position and prevent possible complications and symptoms. The following types of plastic surgery are used to eliminate diastasis.
- Tension technique using patient tissue. The specialist removes excess connective tissue and sews the edges of the muscles together. This technique is used least often, because... relapses often occur after it
- Tension technique using an endoprosthesis. The same removal of excess tissue and suturing of muscles, but at the same time strengthening is performed using a polypropylene prosthesis
- Tension technique with installation of an endoprosthesis. An implant is installed under the area of discrepancy, acting as a barrier and replacing weakened tissue.
- Combined technique. Is a combination of both types of techniques
The surgeon chooses the method of treating diastasis, taking into account the characteristics of the patient’s body, his state of health and the degree of development of diastasis. The end of the rehabilitation period after surgery occurs within 1-3 months. During this time, you need to follow a healthy diet and wear a special bandage that reduces the load on the muscles undergoing surgery.
Preventive measures
To reduce the risk of complications, it is very important to follow professional recommendations for the prevention of diastasis.
- Compliance with the principles of healthy eating
- Active lifestyle
- Strengthening muscles, including the abdominal cavity and lower back
- Systematic moderate, not too severe physical exercise. loads
- Elimination of heavy lifting
- Strengthening the diaphragm
- Maintaining an optimal weight that does not exceed the norm
In the process of bearing a child, it is necessary to use special oils, creams and ointments that stimulate tissue elasticity. After the birth of a child, you should carefully monitor your abs in order to identify pathology in time and, if any problems arise, consult a doctor to prevent complications from developing.
Elimination of diastasis in its initial stage of development is carried out successfully and does not require serious efforts from the patient.
Doctor contact form
Ask your doctor a question
Combination of diastasis with hernias
It should be borne in mind that diastasis is not a hernia. Due to the absence of a hernial orifice, through which abdominal organs can fall out and become pinched, there is no threat to human health. However, the combination of diastasis with hernias (umbilical, linea alba) is quite common. During stage III expansion, they are constant companions. In addition, when a hernia recurs, diastasis often acts as an unfavorable factor. Therefore, during surgery for a hernia, correction of diastasis is necessary.
At any stage of the disease and the presence of concomitant ventral hernias
– their simultaneous correction is always performed.
If there are concomitant diseases of the abdominal and pelvic organs (gastrointestinal tract disease, ovarian cyst, etc.), if the patient wishes, these problems can also be eliminated using laparoscopic access. At the same time, cholecystectomy, removal of fibroids, ovarian cysts, endometriosis, etc. can be performed.
Postoperative period
Surgical treatment of diastasis of the rectus abdominis muscles using tension plasty without a mesh implant implies a longer recovery. The patient is prohibited from lifting weights (more than 10 kg), as well as from playing sports for the first three months. In addition, the patient is considered disabled for a long time.
After minimally invasive surgery, the person operated on can get out of bed on the first day. Immediately after the intervention, a special bandage is put on, which should be worn for 1.5 months. 2 days after the operation, the patient can leave the clinic on her own. After 14 days, you can begin to gradually return to normal life. 2 months after surgery, a person can begin to play sports.
To obtain the best cosmetic effect, it is not recommended to expose the suture area to ultraviolet irradiation (tanning) for a year. After 6 months you can become pregnant and give birth.
Recovery after surgery
- After endoscopic interventions, patients stay in the hospital for no more than 2-3 days and return to everyday life very quickly;
- With open operations, the time frame for returning to a normal lifestyle is extended, but in a number of situations they are simply necessary for the patient.
The next stage after surgery is wearing a postoperative bandage for up to 6 months. As a result, such complex treatment allows you to get rid of the aesthetic problem and prevents further progression of the disease.
Cost of treatment
Free treatment under compulsory medical insurance policy
A type of social insurance for citizens of the Russian Federation, which provides guarantees of free medical care in the detection of surgical diseases.
Quota treatment (VMP)
Providing medical care for the most severe diseases of the gastrointestinal tract, requiring the mandatory use of expensive instruments and/or the use of complex surgical techniques.
Treatment on a paid basis
It assumes the possibility of receiving medical care for any surgical disease, regardless of the presence of a compulsory medical insurance policy, without the need to complete additional documents and obtain a quota, for citizens of all countries of the world.