Microtia and atresia of the external auditory canal
refer to developmental anomalies of the osteocartilaginous skeleton of the external ear. According to statistics, out of approximately 10 thousand children in the world, one is born with congenital pathologies in this area. These changes relate to the so-called disembryogenesis - disturbances in the formation and formation of organs during intrauterine development. Accordingly, the main factors influencing the occurrence of microtia and atresia are effects damaging the embryo - toxic, infectious, less often mechanical, usually in the early stages of pregnancy. The most severe changes occur when the embryo is exposed to a pathological factor before 7 weeks; after the third month, pathology of the middle ear and external auditory canal (atresia) occurs much less frequently; the formation of the auricle is completely completed by the 7th month of intrauterine development; after this period, microtia cannot occur.
What is microtia
Microtia of the auricle is a congenital underdevelopment of the auricle or its absence (Wikipedia). According to various sources, it occurs once every 6,000-10,000 children born. More common in boys than girls. It is more often unilateral than bilateral. One-sided, in turn, is more often on the right than on the left.
According to ICD-10, it belongs to section Q17.2 “Other congenital anomalies (malformations) of the ear. Microtia."
Interesting fact
The incidence of microtia varies from country to country. For example, in Kazakhstan or Mexico, underdevelopment of the auricle is more common than, say, in Switzerland. What this is connected with (with the genetic characteristics of nations, ecology, or for some other reasons) is not yet known.
Degrees of microtia
I degree - as a rule, the auricle is preserved, but reduced in size or slightly deformed. In this case, usually the structures of the middle ear and the auditory canal are preserved, the latter may be narrowed.
II degree – the auricle is underdeveloped. Most often, the ear canal is completely closed or stenotic.
III degree - in place of the auricle there is a so-called rudiment in the form of a skin-cartilaginous ridge with the lobe preserved or not. As a rule, there is complete bony atresia of the auditory canal. The middle ear bones may be intact but deformed or reduced in size. This is the most common form of ear microtia.
IV degree (anotia) – complete absence of any education. Accompanied by complete atresia and disruption of the structures of the middle ear.
CLASSIFICATION OF EAR DEFECTS
The different sections of the ear can be recognized as specific "aesthetic subunits" requiring attention to specific anatomical contours and functional needs. There are congenital and acquired deformities. Acquired ear defects can be distributed as follows:
1. End-to-end
- Total
- Subtotal
- Partial
- Curl
- Curl + anti-helix
- Adjacent anatomical formations
- earlobes
2. Non-through
- Skin + cartilage
- Skin
Causes of microtia
The causes of microtia have not been fully elucidated: in some cases it lies in genetics (with syndromes), in others it is assumed that it is a combination of factors: genetics, impaired blood flow, or certain diseases/medications during pregnancy (3-8 weeks).
I found this genetic test: genetic panel for syndromic microtia. This is not a recommendation to do research, but simply information that such a thing exists. If anyone has taken a similar test, please share the results in the comments.
Types of operations for microtia
There are two directions for correcting microtia of the auricle:
- Reconstruction – recreating the ear as a part of the body.
- Prosthetics is the replacement of the auricle with a removable ectoprosthesis made of artificial material. Most often used when it is impossible or unwilling to carry out reconstruction.
Next we will talk about existing methods in each direction.
Reconstruction of the auricle
Reconstruction of the auricle, in turn, has two directions:
- Reconstruction using autologous (own) tissues. With this method, the frame of the auricle is made from the patient’s costal cartilage and implanted under the skin.
- Reconstruction using artificial materials (implants). In this case, an implant made of artificial material is used as a shell frame: silicone or porous polyethylene (trademarks MEDPOR, SU-POR, OMNIPORE). The frame is either implanted under the skin or covered with a flap of skin.
Reconstruction of the concha from autocartilage
Formation of a shell from costal cartilages covered with skin. The patient's cartilage is removed from 3-4 ribs, from which the ear frame is cut out and sewn together directly during the operation according to a pre-compiled template, which is then implanted under the skin. The patient walks like this for about six months. Then, in one, two or three operations (there are several technologies), the ear is protruded, the lobe and tragus are corrected.
✔ Pros:
- Natural material from our own tissues.
- The ear is a complete part of the body.
✔ Cons:
- 2-4 operations over 6-18 months.
- Poor aesthetics (difficult to replicate the shape of the second ear).
- A long and painful recovery period (very! according to the reviews of those who went through it).
- Often the shell loses its shape over time and dissolves.
- A scar on the skin at the bottom of the chest.
- There is a possibility of deformation of the chest, from which cartilage will be removed.
- Age of surgery after 7-9 years (that is, after the child goes to school).
- There are few surgeons who successfully perform such operations with relatively good cosmetic results.
Conch reconstruction using an artificial implant
This method was developed by American plastic surgeon John Reinisch in 1991. Reconstruction of the auricle is performed on the basis of a frame made of artificial material. The material most often used is medical porous polyethylene (trademarks MEDPOR, SU-POR, OMNIPORE), as well as silicone (but there is very little information about this, I only found it from a plastic surgeon from Moscow - T.Z. Chkadua). There are several techniques: for example, preliminary stretching of the skin and then placing a frame there; but more often it is covered with a flap of leather taken from another place. During healing, the patient’s tissues grow into the pores of the implant, as a result the ear is nourished by blood vessels, acquires sensitivity and becomes a full-fledged part of the body.
✔ Pros:
- One operation (rarely, but sometimes a second may be needed to correct protruding ears, lobes or tragus).
- Age from 3-4 years.
- Quite fast and painless recovery (unpleasant sensations often occur only in the place where the skin was taken).
- The auricle looks more realistic than from autocartilage.
- The ear is a complete part of the body.
✔ Cons:
- The ear is more rigid than the natural one.
- High cost of the operation.
- For several months you will need to take special care of your ear: do not sleep on it, treat it.
- The implant may become damaged and additional surgery will be required. The reason is that the implant itself most often consists of two parts - the base and the curl. During the operation they are connected. But the connection points are the most vulnerable; in the long term they can become displaced or damaged. But developments are underway here too. For example, US surgeon Cheryl Levin performs ear reconstruction using a one-piece implant, which is stronger than the two-piece implants used by other surgeons.
- There is a possibility of death of the tissues covering the ear. There is an opinion that this is the rejection of the implant by the patient’s body (this is how some surgeons hide), but the real reason is that the tissue flap was incorrectly cut by the surgeon himself. As a result, the blood vessels are damaged, the tissue is not nourished properly and dies (turns black). That is why such complications never occur at the hands of some surgeons, but almost without exception at the hands of others.
- There are very few doctors who specialize in this area (and even more so those who perform such operations efficiently with a minimum of complications).
Ear prosthetics
Ear prosthesis on pins. In the first operation, the existing part of the ear is removed and titanium pins are implanted into the bone. A few weeks later, during the second operation, a fastener (special hooks or magnet) is installed, to which a removable silicone prosthesis will be attached.
✔ Pros:
- Quite simple operations.
- The silicone ear will follow the shape of your ear.
✔ Cons:
- Metal structures – pins – are implanted into the head.
- Lifelong daily treatment of areas where metal structures emerge from under the skin is required.
- Infections and inflammations are possible in the area where metal structures emerge from under the skin.
- It is necessary to order a new rubber ear every 2 years (for a fee, of course).
- The sink does not change color in the cold/sunburn (that is, it looks unnatural).
- The ear can become detached and fall at any time (for example, during active play).
- The operation is performed when the bones of the skull are sufficiently strong (most often after the child goes to school).
- In the future, reconstruction of the ear will be impossible (or difficult), since the skin will be scarred and the existing lobe will be cut off. That is, the patient loses the chance for subsequent ear restoration using other methods.
COMPLICATIONS AFTER EAR CORRECTION
- Subcutaneous hematoma is a fairly rare postoperative complication after ear correction. Its signs are quite characteristic: increasing pressing or throbbing pain, which is reported by the patient himself. Diagnosis is not difficult. Treatment consists of inspecting the wound, removing clots and finally stopping the bleeding.
- Epidermal blisters appear on the anterior surface of the auricle and along the edge of the helix. This type of complication occurs when there is excessive traumatic detachment of the skin from the cartilage, as well as the patient’s tendency to allergic reactions.
- Hypertrophic and keloid scars are more often observed after operations with excision of the skin of the postauricular fold and are rare in our practice, since we use gentle incisions with subsequent redistribution of excess skin.
- Ligature fistulas can develop with any type of intervention using internal permanent sutures. We use absorbable threads, which extremely rarely cause this type of complications.
- Recurrence of protrusion occurs when the degree of deformation and, consequently, methods for its correction are incorrectly assessed.
Should I have surgery for microtia?
Arguments for"
✔ Psychological comfort
A person may feel more comfortable with a missing body part than without it.
✔ Sound Capture
The shape of the shell helps to capture and direct sound to the middle ear, thereby improving overall hearing.
✔ Sound source
Relevant for those who have an ear canal (natural or artificial). Having hearing on both sides helps to navigate where the sound source is coming from: right or left. But our space is at least three-dimensional. This is where the complex shape of the shell comes to the rescue, helping our brain to recognize the direction of sound along the top-bottom and front-back axes. That is, full orientation in three-dimensional sound space occurs in conjunction with the presence of hearing on both sides and the presence of shells on both sides. And what is very important is that the sooner the entire system begins to function fully, the greater the chance that the brain will not lose the ability intended by nature to recognize the location of the sound source.
✔ Ear canal protection
Relevant for those who have an ear canal (natural or artificial). The auricle will serve as additional protection for the ear canal from dust and foreign objects.
Arguments against"
List of reasons that may serve as a reason to refuse the operation:
✔ Anesthesia.
✔ Complications are possible (with any method).
✔ Lack of the desired aesthetic effect.
✔ Cost of the operation.
✔ The problem of choosing a surgeon.
You can find a list of doctors who operate for microtia at this link.
Conclusion
Should I have surgery for microtia? If you do, which one?
There is no right answer. I tried to collect as much information as possible to highlight the possible pros and cons. The rest is up to you to decide for yourself or for your children.
ANATOMY OF THE EAR AND CORRECTION OF THE EARS
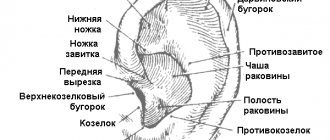
The contours and relief of the auricle differ from person to person in a variety of variations. The auricle is a peculiarly shaped cartilaginous funnel, the bottom of which passes into the external auditory canal. The shell is distinguished between the outer (front) surface - concave and medial (posterior), the surface facing the skull - convex. The “skeleton” of the upper two-thirds of the shell is elastic cartilage, which gives the auricle an extremely complex shape. The thickness of the ear cartilage varies: it is narrower at the free edge and much thicker near the external auditory canal. This has to be taken into account when performing some interventions related to cartilage thinning. The cartilaginous frame of the outer ear is covered with thin skin, which is intimately fused with the perichondrium on the anterior (outer) surface and is located more freely (due to the presence of subcutaneous fatty tissue) on the posterior (inner) surface of the ear. In the lower part of the ear - the ear lobe or lobe - there is no cartilaginous base. The free edge of the shell, folded over its front surface, forms a curl. The anterior end of the helix, located above the external auditory canal, is called the helix. Its lower end is called the caudal section, which passes into the earlobe.
Parallel to the helix on the concave surface of the shell there is a second elevation - the antihelix, which limits the depression in the middle part of the auricle, called the concha proper (concha), which continues into the external auditory canal. The antihelix diverges at the top, forming two legs - the lower (anterior) and upper (posterior), between which there is a triangular fossa.
The helix and antihelix are separated by the scaphoid fossa.
Anterior to the antihelix is the recess of the auricle, divided by the helix into two sections. In front, the recess is limited by a protrusion - the tragus, and behind - by the anti-tragus. The tragus and antitragus are separated by a notch. Rice. 1
- Lobe
- Intertragal notch
- Tragus
- External auditory canal
- Front notch
- Helix leg
- The ascending part of the curl
- Medial (lower) leg of the antihelix
- Triangular fossa
- Horizontal part of the curl
- Lateral (upper) leg of the antihelix
- Scaphoid fossa
- Anti-curl
- Curl
- Ear tubercle (Darwin's tubercle)
- Descending part of the helix
- Antitragus
- Conha
- Shell cavity
- Postauricular sulcus
- Skaf
- Front (outer) surface
- Back (inner) surface
Rice. 2
The ear-head angle is normally 30⁰. The scaphoconchal angle is between the plane of the concha eminence and the antihelical part of the shell; it is normally 90°.
PHOTO OF EAR CORRECTION
If you are interested in ear correction, photos before and after surgery at the Abrielle Aesthetic Surgery Clinic.
You can look here.